

A society can survive a bad year. It can absorb a recession, a delayed generation, or a temporary decline in births. But when fewer children are born year after year, across countries and cultures, one has to wonder: Is there something about modern life that is becoming incompatible with having babies?
The Global Fertility Shift
What we are experiencing is not a brief demographic wobble or a temporary dip in population. Fertility decline has become a defining feature of the modern world.
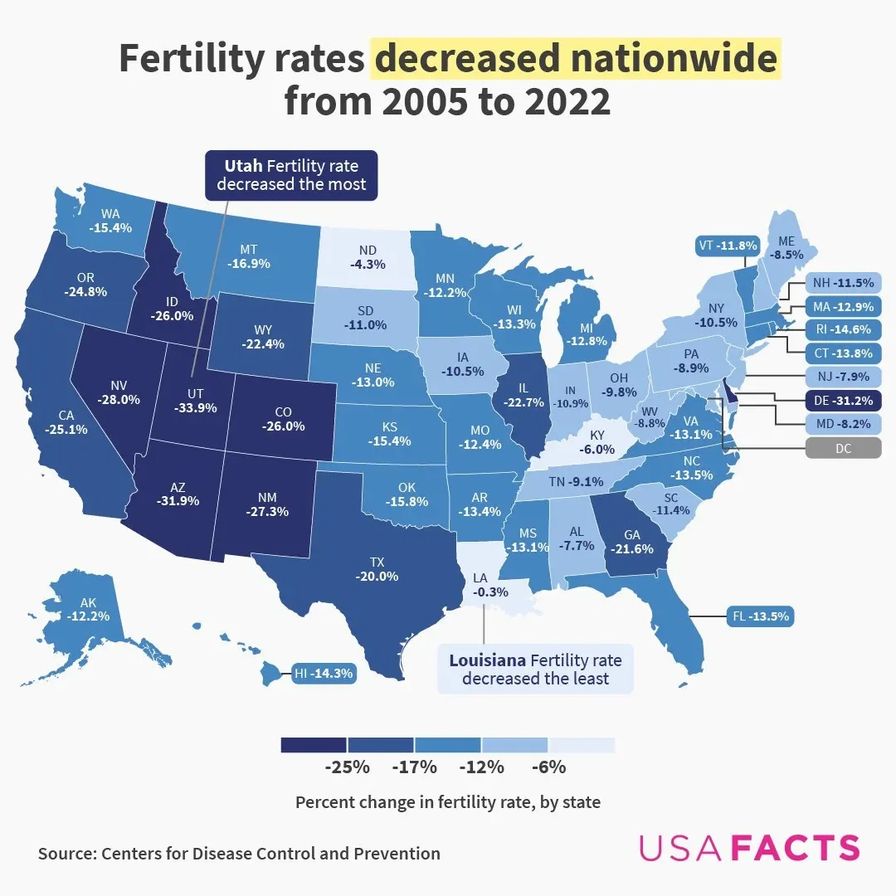
For more than a decade, fertility rates in the United States have remained well below what is needed to sustain the population over time. Data from the CDC’s National Center for Health Statistics places the U.S. total fertility rate at about 1.63 births per woman, well below the replacement level of 2.1. Even when the number of births rises slightly from one year to the next, the larger pattern remains difficult to ignore: Americans are having fewer children than previous generations.
Globally, the pattern is even more striking. According to the United Nations’ World Fertility 2024 report, 55 percent of countries had fertility rates below replacement level in 2024. This means that 68 percent, more than two-thirds of people, now live in places where fertility has fallen below the level needed to replace the population over time.
But is this an unprecedented disaster?
Not exactly. Low fertility does not lead neatly or immediately to collapse, but demographic decline does place pressure on the systems society depends on… especially when the decline persists long enough to reshape the balance between generations.
Why Demography Matters
Demographic decline rarely announces itself like a war. It begins quietly: fewer marriages, fewer children, more aging parents with fewer adults to care for them, more schools closing, more towns emptying. At first, the problem can look manageable. A country can borrow, automate, import labor, raise retirement ages, or ask the young to work harder and wait longer.
But a sustained decline in fertility affects far more than individual family size. It changes the structure of communities and the long-term stability of social systems. Fertility rates shape tax bases, economies, workforces, elder care, healthcare systems, schools, and more.
The pressure becomes especially visible in pay-as-you-go systems like Social Security, where current workers fund benefits for current retirees. According to Social Security Administration historical data, there were 16.5 covered workers for every Social Security beneficiary in 1950. Today, that ratio is closer to three workers per beneficiary, and the strain is already showing. The 2025 Social Security Trustees Report projects that the Old-Age and Survivors Insurance Trust Fund will be depleted in 2033; if Congress does not act, continuing income would be sufficient to pay only 77 percent of scheduled benefits at that time.
This does not mean older adults are a burden. Longer life is one of humanity’s great achievements, but the issue is imbalance. A society with fewer young people and more older adults must eventually answer difficult questions about who will care for the aging, who will staff essential industries, and who will support systems designed around a broader base of working-age adults.
Lessons From History
Ancient societies did not track fertility the way modern demographers do, but they did understand that society depends on generational replacement.
Sparta offers one historical example of what happens when a population base shrinks too much. Spartan society depended on a narrow class of full citizens, the Spartiates, who sustained its military and political order. Modern scholarship describes the Spartiate population falling from roughly 8,000 to fewer than 1,000 over the Classical and Hellenistic periods.
Sparta’s decline had many causes, including war, inequality, land concentration, and political rigidity. But the shrinking Spartiate population weakened the very structure that had made it powerful. The city still had people, but what it lacked was enough citizens to sustain the military and political order on which Sparta depended.
The lesson is not that low fertility automatically destroys a civilization, but something more unsettling: when a society loses the ability or will to reproduce, every other weakness becomes harder to survive. Debt becomes heavier. Elder care becomes more fragile. Institutions age alongside the people within them and begin to strain under their own weight.
Choice Is Only Part of the Equation
Fertility decline is often discussed in narrow political terms, treated as though it begins and ends with preference. One side frames it as a failure of family values, while another frames it as liberation from outdated expectations. Others may dismiss the issue altogether, arguing that fewer people could ease pressure on the planet. But sustained fertility decline is not simply a moral issue, a woman’s issue, an economic issue, or an environmental issue. As the Sparta example shows, it is a systems issue.
The mainstream explanations are not wrong. Rising cost of living, a volatile housing market, exorbitant childcare expenses, student debt, unstable work, low wages, inadequate parental leave, the state of our healthcare and insurance systems, economic uncertainty, delayed marriage, and the absence of meaningful family support all shape decisions about whether and when to have children. People are also having children later in life, and parenthood is no longer treated as the only path to adulthood, societal contribution, identity, or life meaning.
These factors matter deeply. Many people are making rational decisions within systems that make family life harder than it has traditionally been. But there is evidence that choice is only part of the equation. The other part is the state of human reproductive health.
Over the past several decades, researchers have documented measurable changes in human reproductive health. One of the most widely cited examples is declining sperm counts. A 2023 systematic review and meta-analysis published in Human Reproduction Update looked at data from more than 57,000 men around the world and found that average sperm concentration fell by more than 50 percent between 1973 and 2018. Total sperm count fell by more than 60 percent over over the same period. The authors described the trend as a global concern that warrants further research and public health attention.
And male reproductive health is only half of the equation; women’s reproductive health reflects a similar level of strain. According to the World Health Organization, polycystic ovarian syndrome, or PCOS, affects 10-13 percent of reproductive-age women, while endometriosis affects about 10 percent of reproductive-age women. Both conditions are chronic, often underdiagnosed or delayed in diagnosis, difficult to treat, and associated with significant fertility challenges.
When large numbers of people are navigating hormonal disorders, ovulatory dysfunction, chronic reproductive inflammation, sperm count decline, infertility, or pregnancy loss, fertility decline cannot be understood as a matter of choice alone. A growing share of medically assisted pregnancies adds further nuance to the discussion. According to the latest CDC surveillance data, roughly 1 in 38 U.S. infants born in 2022 was conceived through assisted reproductive technology. Top reasons for utilizing fertility interventions are having children later in life, fertility preservation, navigating infertility struggles, and building families in ways previous generations could not. These technologies are not a cause of fertility decline, but its increasing role in family planning reflects that, for many families, having children now requires more medical assistance, planning, and intervention than the simple “people are choosing fewer children” narrative.

The Exposome: A Wider Lens on Fertility
If reproductive capacity is part of the fertility story, then the next question is what may be affecting it.
That is where the field of exposomics becomes relevant. Exposomics is the study of the exposome: the full range of environmental exposures a person experiences over a lifetime, beginning as early as conception, and how the body responds to them. Rather than looking at one chemical, one product, or one exposure pathway in isolation, exposomics asks a broader question: what is the cumulative impact of the environments we live in?
That question matters deeply for fertility because the concern is not limited to one chemical class or one source of exposure. People encounter potential reproductive stressors through the food they eat, the water they drink, the air they breathe, the environments they move through, and the stressors they carry each day. Some of these exposures involve chemicals in plastics, pesticides, PFAS, flame retardants, cosmetics, cleaning products, textiles, and consumer goods.
Modern infrastructure is also not separate from public health. The rapid expansion of data centers across the United States further introduces pollutants into the environments where we work, live, and farm our food. Even foods that we think are healthy can be seriously harmful due to heavy metal contamination and lack of regulation. For instance, heavy metals found in coal ash, root vegetables, and leafy greens have been shown to cause reproductive damage. Other significant factors involve chronic stress, poor nutrition, metabolic dysfunction, inflammation, sleep disruption, and infections.
Each exposure may be difficult to isolate, but the human body does not experience these inputs one at a time. It experiences them cumulatively, as part of a broader environmental load. This is why fertility decline should be evaluated through a wider lens. No single exposure can explain the whole story, but collectively, these exposures raise a serious public health question: are we evaluating fertility decline in a way that reflects real life?
A Systems Problem Requires a Systems Response
It would be irresponsible to claim that environmental exposures alone are causing fertility collapse. The evidence does not support that kind of simple, one-cause explanation. But it would be equally irresponsible to ignore the growing body of research suggesting that the environments we live in may affect reproductive development and function, especially during sensitive windows such as pregnancy, infancy, childhood, and puberty.
A generation facing rising housing costs, delayed financial stability, limited childcare, chronic stress, environmental exposures, and increasing reproductive health challenges is not making family decisions in a vacuum. These choices are being made inside systems that shape what feels possible, what feels safe, and what the body itself is capable of sustaining.
The point is not to panic. It is to pay attention.
If fertility decline is a signal, then a serious response must look beyond slogans and ask better questions. Are we making family formation economically possible? Are we protecting reproductive health before infertility reaches a crisis point? Are we studying the cumulative impact of exposures across food, water, air, homes, workplaces, and consumer products? Are we holding regulators and industries accountable for the conditions families are expected to navigate?
What Can Be Done?
A serious response to fertility decline should include:
- Reducing avoidable exposures in homes, schools, workplaces, food, water, and consumer products. Families can take steps where possible, such as filtering drinking water, reducing plastic food contact, choosing safer personal care and cleaning products, avoiding unnecessary pesticide use, and supporting cleaner food systems. But exposure reduction cannot fall on individuals alone.
- Making family formation economically and medically possible through affordable housing, paid parental leave, childcare support, flexible work, access to reproductive healthcare, and policies that do not punish parents for having children.
- Advocating for better screening, care, and research for conditions that affect fertility, including PCOS, endometriosis, thyroid dysfunction, metabolic dysfunction, male-factor infertility, recurrent miscarriage, and other reproductive health concerns. These issues should be identified earlier, studied more seriously, and treated as public health priorities rather than private struggles.
- Holding regulators and industries accountable through stronger chemical transparency, safer food packaging, cleaner water standards, pesticide reduction, cumulative-exposure research, and support for organizations like Moms Across America that push for safer food, cleaner environments, and stronger protections for families.
The question is not whether every person should have children. The question is whether we are building a world where the people who want to can, and where human reproduction is protected as a basic marker of public health. “Reproductive rights” now has a new meaning; no longer should we see these words and think, the right to abortion. Abortion is a moot point if American women cannot get pregnant.
This is demonstrated by data from 2023, in which the U.S. had just over one million abortions, while CDC infertility data suggest roughly 8 million women of reproductive age experienced impaired fertility or difficulty carrying a pregnancy. Infertility affects roughly eight times more women than the number of women who do not want/abort.
If we are willing to look beyond the surface, fertility collapse may be telling us something profound: not just about birth rates, but about the health of the world we have built.